I had downloaded The Twelve to my iPad for a trip, but didn’t get to it, and sort of forgot it was there until my son mentioned he was listening to it on audio-books, and it was good, maybe even better than the first book in the trilogy, The Passage. He had loaned me The Passage several years ago when it came out, and as soon as I finished, I got on the list to download as soon as the next book came out – it was that good.
Cronin’s gift is an ability to create a future world entirely different from our own, with a devastating enemy – the virals – who, literally, are us, transformed. Cronin can make the enemy terrifying, destructive, truly horrifying – and can make them also captive to their repugnant nature and even pitiable. I think that is an amazing dance for an author to accomplish.
The setting is post-apocalyptic USA; the government had a sector working on a secret weapon which – of course – was not able to be contained, creating 12 super vampire-like creatures called Virals, who in turn create hordes of minions. This volume, The Twelve, is set more than 100 years later, but shifts back to earlier times to help us understand how this disaster occurred, and how characters relate back to the earliest times of the disaster. The populations live in fear of sudden attacks; one family, out on a picnic, are almost totally wiped out by an eclipse for which the Virals were prepared – and the families were not.
As I read his books, I find them very cinematic, but, as my son and I discussed, too complex for a movie; it would need a gritty HBO series like The Wire, or OZ, or Deadwood to capture the subtleties, the nuances that make this a best-selling series. The heroes and heroines are all make for the screen, their relationships – and inter-relationships – make them interesting, and then, as we learn more, interesting again. We never know enough to make a final judgement on any character; the characters are complex and the relationships obscure until the author chooses to reveal. It makes it fun to try to spot them before he tells us. I missed a couple!
Although it can be read as a great-adventure stand-alone, you’ll be happier if you read The Passage before you read The Twelve. If you have a problem with postponing gratification, you might want to wait until the third and conclusive volume of the trilogy is published – and that may be a year or so.
July 13, 2013
Posted by intlxpatr |
Adventure, Books, Character, Community, Fiction, Health Issues, Living Conditions, Political Issues, Relationships, Social Issues, Survival | Post Apocalypse, virals |
Leave a comment
AdventureMan and I are not vegetarian; we eat a lot of fish and we try not to eat a lot of beef, pork or lamb. Lamb isn’t so much of a problem here in Pensacola – you don’t even see it on the menu that often. But pork – and beef – are everywhere.
Once a year I have a burger. Really. AdventureMan will order a burger more often, and I might take one bite here and there, but once a year, usually around the 4th of July, I will have my onec-a-year burger.
(Do you have any idea how many calories one burger has in a resturant? It’s all the extras, the bacons, the sauces, the fried onions, it can be two days worth of calories in ONE burger. It can seriously clog your veins in as little as two hours after you eat one. )
Because I only have one, it has to be a really really good one. I got hooked on Red Robin burgers back in university; then, Red Robin was really a college beer joint that served really good burgers. I ordered the A-1 Peppercorn Burger, but when it came, it came on some kind of a roll 😦 not the real hamburger bun.

It was everything I had hoped for – and more. The meat was cooked perfectly, not overdone; juicy and not greasy. The bacon (yes, yes, I did. It’s just once a year) was crisp. The sauce was peppery, just the way I like it. And yes, I ate the onion rings, too.
Now I’m good for another year 🙂
July 12, 2013
Posted by intlxpatr |
Aging, Cooking, Cultural, Eating Out, Food, Health Issues, Restaurant | hamburger, Red Robins |
Leave a comment
From the Daily Mail (UK)
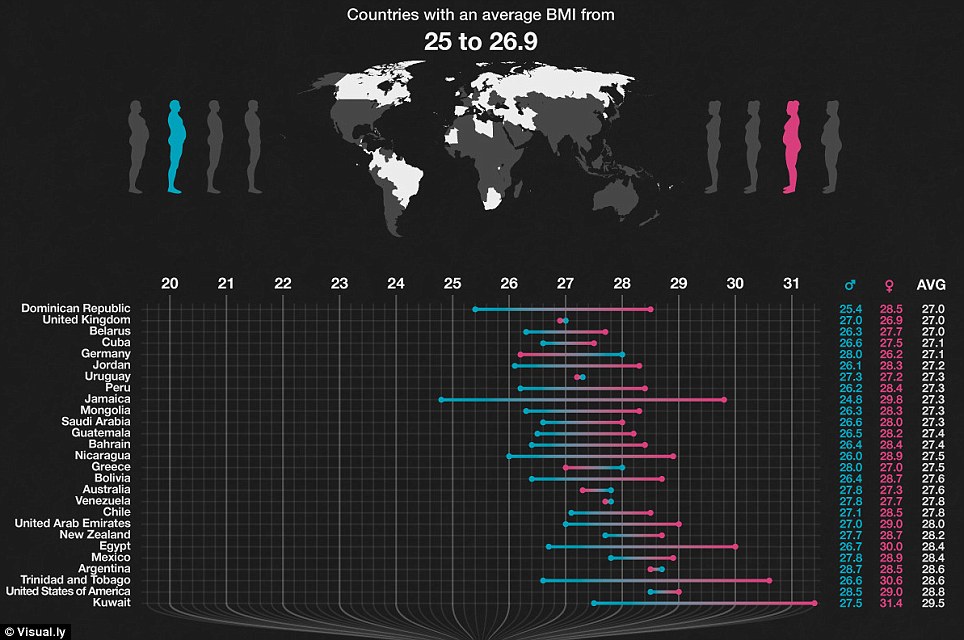
The countries which contain the heaviest and lightest citizens can be revealed today.
This extraordinary graphic shows the average body mass index values for adults around the globe – with some surprising results.
With its wealthy society and love of fast food outlets, many would place the U.S. at the top of the list.

But it is pipped to first place in the body mass index chart by Kuwait. The Arab state has an average body mass index of 27.5 for men and 31.4 for women.
This beats America in second place which averages 26.5 for men and 29 for women.
From UPI:
Mexico is world fattest nation, United States No. 2
UNITED NATIONS, July 10 (UPI) — Officials at the U.N. Food and Agricultural Organization say Mexico with a 32.8 percent adult obesity rate is the most overweight of the industrialized nations.
Previously, the United States with an adult obesity rate of 31.8 percent was the world’s fattest nation. Last year, the percentage of U.S. adults overweight went down slightly.
A report by the FAO said Mexico’s widely available inexpensive junk food and penetration of U.S. fast-food chains combined with a more sedentary lifestyle all contributed to Mexico’s bulging waistline.
About 70 percent of Mexican adults are overweight, while childhood obesity tripled in a decade and about a third of teenagers are overweight as well, the Global Post said.
Weight-related diabetes claims 1-of-6 one of Mexican adults — or 70,000 people a year — suffering from the disease each year, the report said.
July 10, 2013
Posted by intlxpatr |
Cross Cultural, Cultural, Eating Out, Food, Health Issues, Kuwait | BMI, Mexico, Obesity, United States |
Leave a comment
“I miss the highs. . . ” my friend said – just before she went off her meds.
I totally understood what she was saying. We belonged to a quilting group, and when she was beginning a manic phase, she produced knock-out quilts, quilts combining colors in unusual ways, and she could stay up all night to finish one. She was a lot of fun to be around, totally up and enthusiastic and creative. As the phase progressed, however, she got thinner and thinner, fell in love with the wrong men, and I always knew when she was just about to crash because she looked fabulous – new clothes, lots of shoes, and she talked a mile a minute.
Then the crash. Her biggest fear was the credit card bills; when she was on a high, she felt like it didn’t matter. When she slid into depression, it was complicated by the fact that she had real things to be depressed about – STDs, huge bills, and concerns at her workplace and her security clearance.
As long as she was on her meds, she was fine, but the medications made her feel sluggish; she said even colors were less colorful on her meds. She said it was like spending your life underwater, where things were not so clear. She said it was dull.
It’s easy, when you are not bi-polar, to say “stay on your meds.” It’s really hard to do it when the meds can make you feel like you are living in a prison.
My friend recommended a book by Kay Redfield Jamison called An Unquiet Mind. It was one of the most helpful books I have ever read, helping me to understand just how hard it is to give up the mania in spite of the huge price you pay for it with the depressions.
I hope my friend is still alive.
This article is from AOL Health News:
4 Surprising Signs of Bipolar Disorder
Fewer than half of Americans with bipolar disorder are properly diagnosed and treated, recent research shows. Could you spot bipolar symptoms – in yourself or in someone close to you?
Many people with bipolar disorderdon’t even know they have it.
Fewer than half of people in the United States who show classic signs of bipolar disorder actually get diagnosed and treated, says a recent Archives of General Psychiatry report on a survey of more than 61,000 adults in 11 countries — the United States, Mexico, China, Japan, Brazil, Colombia, India, Lebanon, Bulgaria, Romania, and New Zealand. Bipolar patients in lower-income nations get even less treatment — in some cases, as few as 25 percent receive help.
Compared to the other 10 countries studied, the United States had the highest rate of bipolar disorder (4.4 percent of those surveyed fell somewhere on the bipolar spectrum). India had the lowest (0.1 percent). Overall, about 2.4 percent of those interviewed in the face-to-face survey could be classified as having bipolar disorder.
Bipolar Disorder’s Most Surprising Symptoms
It may be buzz-worthy these days, but many people don’t fully understand bipolar disorder and the symptoms that can lead to proper diagnosis and treatment. Bipolar, also sometimes called manic-depressive disorder, is characterized by shifts from extreme highs (known as mania) to emotional lows (depression), with “normal” moods in between.
It’s bipolar disorder’s manic phase that most sets it apart from other common mental health issues, such as depression and anxiety. While many people associate mania with high energy and exaggeratedly good moods, these other key symptoms are more subtle:
- Reckless spending. If a friend is blowing her paycheck on shopping sprees she can’t afford, watch out. A person in a manic phase of bipolar disorder is more likely to take big risks, including spending splurges that can lead to mountains of unmanageable debt.
- Super-charged sex drive. A sudden revving up of a person’s sex drive, obsessively thinking or talking about sex, or engaging in sexual encounters he otherwise wouldn’t (like a one-night stand or sex with someone he doesn’t know well) are all symptoms of hypersexuality, another less-obvious mania clue.
- Alcohol or drug abuse. These often go hand-in-hand with manic episodes: As many as 60 percent of people with bipolar disorder have abused alcohol or drugs at some point in their lives. Depressants such as alcohol or pain pills can send a person with mania straight into depression, while stimulants like cocaine can have the opposite effect.
- Skimping on shut-eye. Little need for sleep is another red flag that a person may be having a manic episode.
Keep in mind that bipolar disorder can vary greatly in severity, and not everyone experiences every symptom. In fact, some patients experience hypomania, a less mild form of mania. But even hypomania, if left untreated, could spin into depression or develop into full-blown mania.
One important takeaway from the Archives study is that across all countries, patients with bipolar disorder faced challenges in their daily lives and were at increased risk of such health problems as panic attacks, substance abuse, and suicide. Untreated bipolar disorder can also lead to troubled relationships with friends and family and problems at work. If you’re concerned about yourself or a friend or loved one, get more information here on the best treatments for bipolar disorder.
Last Updated: 08/08/2012
July 9, 2013
Posted by intlxpatr |
Arts & Handicrafts, Character, ExPat Life, Financial Issues, Germany, Health Issues, Relationships | bipolar disorder, manic-depression, Mental health issues |
3 Comments
Technically, those who are ill are not required to fast, but my diabetic friends have said they can fast if they do it cautiously. I found this fascinating report on diabetics and fasting, particularly Ramadan fasting. You can reference the website Islam.ru.
Source:By: Fereidoun Azizi, MD, and Behnam Siahkolah, MD,/ Intl. Journal of Ramadan Fasting Research* / islamicity.com/October 31/2002 , res
Several of the world’s great religions recommend a period of fasting or abstinence from certain foods. Of these, the Islamic fast during the Muslim month of Ramadan is strictly observed every year. Islam specifically outlines one full month of intermittent fasting. The experience of fasting is intended to teach Muslims self-discipline and self-restraint and remind them of the plight of the impoverished. Muslims observing the fast are required to abstain not only from eating and drinking, but also from consuming oral medications and intravenous nutritional fluids.
The month of Ramadan contains 28 days to 30 days. The dates of observance differ each year because Ramadan is set to a lunar calendar. Fasting extends each day from dawn until sunset, a period which varies by geographical location and season. In summer months and northern latitudes, the fast can last up to 18 hours or more. Islam recommends that fasting Muslims eat a meal before dawn, called “sahur.” Individuals are exempt from Ramadan fasting if they are suffering from an illness that could be adversely affected by fasting. They are allowed to restrain from fasting for one day to all 30 days, depending on the condition of their illness. People diagnosed with diabetes fall into this category and are exempt from the fasting requirement, but they are often loathe to accept this concession. Physicians working in Muslims countries and communities commonly face the difficult task of advising diabetic patients whether it is safe to fast, as well as recommending the dietary and drug regimens diabetics should follow if they decide to fast. The lack of adequate literature on this subject makes it difficult to answer these questions. To judge correctly whether to grant medical permission to fast to a diabetic patient, it is essential physicians have an appreciation of the effect of Ramadan fasting on the pathophysiology of diabetes mellitus. In this article, we first review principles of carbohydrate metabolism and alterations of certain biochemical variables in diabetics observing Ramadan fasting. We then overview current medical recommendations that allow certain diabetic patients to fast and outline terms for diabetic patients, particularly IDDM patients, who should not fast but insist on fasting.
THE PHYSIOLOGICAL STATE OF DIABETICS DURING RAMADAN
Carbohydrate metabolism during Ramadan fasting in healthy persons
The effect of experimental short-term fasting on carbohydrate metabolism has been extensively studied (1,2). It has been uniformly found that a slight decrease in serum glucose to 3.3 mmol to 3.9 mmol (60 mg/dl to 70 mg/dl) occurs in normal adults a few hours after fasting has begun. However, the reduction in serum glucose ceases due to increased gluconeogenesis in the liver. That occurs because of a decrease in insulin concentration and a rise in glucagon and sympathetic activity (3). In children aged one years to nine years, fasting for a 24-hour period has caused a decrease in the blood glucose to half of the baseline figure for normal children of that age group. In 22% of these children, blood glucose has fallen below 40 mg/dl (4). Few studies have shown the effect of Ramadan fasting on serum glucose (5-9). One study has shown a slight decrease in serum glucose in the first days of Ramadan, followed by normalization by the twentieth day and a slight rise by the twenty-ninth day of Ramadan (6). The lowest serum glucose level in this study was 63 mg/dl. Others have shown a mild increase (7) or variation in serum glucose concentration (8,9), but all of them fell within physiological limits (6). From the foregoing studies, one may assume that the stores of glycogen, along with some degree of gluconeogenesis, maintain normal limits of serum glucose when a fast follows a large pre-dawn meal. However, slight changes in serum glucose may occur in individuals depending upon food habits and individual differences in metabolism and energy regulation.
Body weight during Ramadan fasting
(a) In normal subjects:
Weight losses of 1.7 kg. (10), 1.8 kg. (11), 2.0 kg. (12) and 3.8 kg (13) have been reported in normal weight individuals after they have fasted for the month of Ramadan. In one study that was over-represented by females, no change in body weight was seen (14). It has also been reported that overweight persons lose more weight than normal or underweight subjects (12).
(b) In diabetics:
A review of literature shows controversy about weight changes in diabetics during Ramadan.(6,15-24). In one group of studies, patients had an increase in their weight (17,21). In another group, there were no change (15,19,22,23) or a decrease (6,16,18,20,24) in body weight. While no food or drink is consumed between dawn and sunset during the month of Ramadan, there is no restriction on the amount or type of food consumed at night (23,25). Furthermore, most diabetics reduce their daily activities (15,23) during this period in fear of hypoglycemia. These factors may result in not only a lack of weight loss, but also a weight gain in such patients(26). (See later discussion about nutrition and physical activity.)
Blood glucose variations during Ramadan fasting in diabetics
Most patients show no significant change in their glucose control (3,23,24,27). In some patients, serum glucose concentration may fall or rise (28-30). This variation may be due to the amount or type of food consumption, regularity of taking medications, engorging after the fast is broken, or decreased physical activities. In most cases, no episode of acute complications (hypoglycemic or hyperglycemic types) occurs in patients under medical management(9,15,16,22), And only a few cases of biochemical hypoglycemia without clinical hazards have been reported (17,19,25).
Other parameters of diabetes control during Ramadan fasting
In general, HbAIC values show no change or even improvement during Ramadan (15-18,20,22,23,25,27,28,32). Only two studies have reported slight increases in glycated hemoglobin levels (19,31). However, one report has emphasized the same increase in non-fasting patients as fasting patients (31), and the other has shown a return to initial levels immediately after the month of Ramadan (19).
The amount of fructosamine (17,22,24,30,32), insulin, C-peptide (23,30) also has been reported to have no significant change before and during Ramadan fasting.
Energy intake and serum lipid variables during Ramadan fasting in diabetics
The amount of Energy (calorie) intake have been reported in some of the literature, indicating a decrease in energy intake (24,28).
Most patients with non-insulin dependent diabetes mellitus (NIDDM, diabetes type II) and insulin dependent diabetes mellitus (IDDM, diabetes type I) show no change or a slight decrease in concentrations of total cholesterol and triglyceride (15-19,27,28,32). Increase in total cholesterol levels during Ramadan seldom occurs (23). As in healthy persons (33-36), few studies have reported increases in high-density-lipoprotein (HDL) cholesterol in diabetics during Ramadan (18,19,27). One report indicates an increase in low-density-lipoprotein (LDL) cholesterol and a decrease in HDL-cholesterol (28). Until there is a standardization of diabetes Ramadan research in three fundamental factors — the Three D Triangle of drug regimens, diet control and daily activity — the benefits or hazards of Ramadan fasting on diabetics serum lipids is unclear.
Other biological parameters during Ramadan fasting in diabetics
Serum creatinine, uric acid, blood urea nitrogen, protein, albumin, alanine amino-transferase, aspartate amino-transferase values do not show significant changes during the fasting period(15,17,32). Slight non-significant increases in some biological parameters may be due to dehydration and metabolic adaptation and have no clinical presentation.
FASTING GUIDELINES TO DIABETICS
During the last two decades, a better understanding of pathophysiological changes during Ramadan fasting in diabetic patients has provided a few guidelines on how to advise diabetics who want to fast. Physicians working with Muslim diabetics should employ certain criteria to advise their patients regarding the safety of Ramadan fasting.
The following criteria should be helpful in making such a decision (20,37):
Forbid fasting in:
- All brittle type I diabetic patients;
- Poorly controlled type I or type II diabetic patients;
- Diabetic patients known to be incompliant in terms of following advice on diet drug regimens and daily activity;
- Diabetic patients with serious complications such as unstable angina or uncontrolled hypertension;
- Patients with a history of diabetic ketoacidosis;
- Pregnant diabetic patients;
- Diabetic patients will inter-current infections;
- Elderly patients with any degree of alertness problems;
- Two or more episodes of hypoglycemia and/or hyperglycemia during Ramadan.
Allow fasting in:
- Patients who do not have the aforementioned criteria;
- Patient who accept medical advisement.
Encourage fasting in:
-
All overweight NIDDM patients (except for pregnant or nursing mothers) whose diabetes is stable with weight levels 20% above the ideal weight or body mass index (body weight, kg/height, meters squared) greater than 28.
EDUCATION OF THE DIABETICS BEFORE RAMADAN
NIDDM patients and IDDM patients who insist on fasting should be given a few recommendations about fasting (16). They should be forbidden from skipping meals, taking medication irregularly or gorging after the fast is broken (26).
The principles of pre-Ramadan considerations are (37):
- assessment of physical well being;
- assessment of metabolic control;
- adjustment of the diet protocol for Ramadan fasting;
- adjustment of the drug regimen e.g. change long-acting hypoglycemic drugs to short-acting drugs to prevent hypoglycemia);
- encouragement of continued proper physical activity;
- recognition of warning symptoms of dehydration, hypoglycemia and other possible complications.
RECOMMENDATIONS DURING RAMADAN FASTING
I. Nutrition and Ramadan fasting:
Dietary indiscretion during the non-fasting period with excessive gorging, or compensatory eating, of carbohydrate and fatty foods contributes to the tendency towards hyperglycemia and weight gain (21,23). It has been emphasized that Ramadan fasting benefits appear only in patients who maintain their appropriate diets (24,38,39). Thus, in order to optimize control, diabetics must be reminded to abstain from the high-calorie and highly-refined foods prepared during this month (38).
II. Physical activity and Ramadan fasting:
Several studies indicate that light to moderate regular exercise during Ramadan fasting is harmless for NIDDM patients (15). It has been shown that fasting does not interfere with tolerance to exercise (40). It should be impressed upon diabetic patients that it is necessary to continue their usual physical activity especially during non-fasting periods (41)
III. Drug regimens for IDDM patients:
Some experienced physicians conclude Ramadan fasting is safe for IDDM patients with proper self-monitoring and close professional supervision (16). It is fundamental to adjust the insulin regimen for good IDDM control during Ramadan fasting. Two insulin therapy methods have been studied successfully:
-
Three-dose insulin regimen: two doses before meals (sunset and Dawn) of short-acting insulin and one dose in the late evening of intermediate-acting insulin (16).
-
Two-dose insulin regimen: Evening insulin combined with short-acting and medium-acting insulin equivalent to the previous morning dosage, and a pre-dawn insulin consisting only of a regular dosage of 0.1-0.2 unit/kg (25).
Home blood glucose monitoring should be performed just before the sunset meal and three hours afterwards. It should also be performed before the pre-dawn meal to adjust the insulin dose and prevent any hypoglycemia and post-prandial hyperglycemia following over-eating.
IV. Drug regimens for NIDDM patients:
Available reports indicate that there are no major problems encountered with NIDDM overweight patients who observe fasting in Ramadan (3). With proper changes in the dosage of hypoglycemic agents there will be low risk for hypoglycemia and hyperglycemia.
The authors of the largest series of patients treated with glibenclamide during Ramadan recommended that diabetics switch the morning dose (together with any mid-day dose) of this drug with the dosage taken at sunset (31).
V. Other health tips for reduction of complications:
-
Implementation of the 3D Triangle of Ramadan — drug regimen adjustment, diet control and daily activity — as the three pillars for more successful fasting during Ramadan.
-
Diabetic home management that consists of:
– Monitoring home blood glucose especially for IDDM patients, as described above;
– Checking urine for acetone (IDDM patients);
– Measuring daily weights and informing physicians of weight reduction (dehydration, low food intake, polyuria) or weight increase (excessive calorie intake) above two kilograms;
Recording daily diet intake (prevention of excessive and very low energy consumption).
-
Education about warning symptoms of dehydration, hypoglycemia and hyperglycemia.
-
Education about breaking fast as soon as any complication or new harmful condition occurs.
-
Immediate medical help for diabetics who need medical help quickly, rather than waiting for medial assistance the next day.
-
Further attention on fasting during the summer season and geographical areas with long fasting hours.
VI. IDDM children and Ramadan fasting:
We do not encourage fasting for IDDM children. However, a few studies demonstrate that fasting is safe among diabetic adolescents. Of these studies, one study concludes that Ramadan fasting is feasible in older children and children who have had diabetes for a long time, and it concludes fasting does not alter short-term metabolic control. Nevertheless, fasting should only be encouraged in children with good glycemic control and regular blood glucose monitoring at home (25).
POST-RAMADAN SUPERVISION OF FASTING DIABETICS
After the month of Ramadan ends, the patients therapeutic regimen should be changed back to its previous schedule. Patients should also be required to get an overall education about the impact of fasting on their physiology (37).
THE RESEARCH METHODOLOGY ON DIABETICS DURING RAMADAN
From a methodological point of view, few research papers on Ramadan fasting are relevant because of the absence of control periods before Ramadan and afterwards, the absence of measurements during each week of Ramadan, a lack of attention to dietary habits, food composition, food value, caloric control, weight changes and the importance of the schedule during circadian periods.
It is recommended that all these factors should be taken into consideration and that all intervening and confounding variables should be under control. It is clear that more work should be done on Ramadan fasting to evaluate physiological and pathological changes with proper research methods (42).
Fasting during the entire month of Ramadan is reserved usually for healthy Muslims. However, many diabetic patients are allowed to fast periodically during Ramadan. The magnitude of periodic total fasting effect on blood glucose and hepatic glucagon depends on the number of fasting days (43), and this should be considered in all Ramadan fasting research activities.
CONCLUSION
The bulk of literature indicates that fasting in Ramadan is safe for the majority of diabetics patients with proper education and diabetic management. Most NIDDM patients can fast safely during Ramadan. Occasional IDDM patients who insist on fasting during Ramadan can also fast if they are carefully managed. Strict attention to diet control, daily activity and drug regimen adjustment is essential for successful Ramadan fasting.
To shed more light on pathophysiological changes in Ramadan fasting, in particular in Muslims diabetics, it is recommended that a multicentric international controlled clinical trial be employed to assess the effect of differences in gender, races, physical activities, food habits, sleep patterns and other important variables on physiologic and pathologic conditions during Ramadan fasting.
July 7, 2013
Posted by intlxpatr |
Food, Health Issues, Ramadan | diabetes, diabetics, fasting |
Leave a comment

I talked AdventureMan into going to see World War Z with me – us and half of Pensacola showed up for the early matinee, and we got the last two seats. I had thought it’s been out for a while and people would be going to see something else, but all the theaters showing it in Pensacola are selling out every show. That doesn’t mean every seat was already filled – a lot of people had bought tickets online but weren’t there. On the other hand, while we got two good seats – they were – LOL – at opposite ends of the row!
World War Z is not a movie where you want to be sitting on opposite ends of the row.
World War Z is Contagion on steroids.
Did you ever see Romero’s 1968 Night of the Living Dead? I used to love scary movies, until I saw that movie. The scary movies were funny, not so scary at all – and George Romero changed all that with this low-budget horror classic. I think I liked it because it had a scientific kind of origin – a virus.
World War Z takes a similar approach, a scientific approach, and it is also very scary because it is hard, very hard, to be scientific and observant when your entire world becomes unsafe, when everything you known has turned to chaos. The zombies aren’t so damaged and tattered as Romero’s zombies, but they have the same herd mentality, a frenzied mob mentality, and an Alien-like skittering and swarming that makes my skin crawl.
I love seeing Brad Pitt as a responsible family man. He does it well. He has to make some very tough decisions in this movie, and you get to see that this sweet family man has another, tougher side.
AdventureMan was glad we went; he also thinks this will be a great computer game. We agreed it was scary because it had some things in it that truly can make life dangerous – you know, political leaders dying en masse, political and social systems dissolving and life becoming a brute struggle for survival with scarce resources . . . having swarming zombies kicks all that up a notch.
Not a movie for anyone under five. Maybe not even ten, if the kids are sensitive, or prone to bad dreams . . .
Our son said we need to read the book; it’s only sort-of like the movie, and has a lot of very edgy things to say about our current political system and leaders. Hmmmm. . . might have to do that.
July 6, 2013
Posted by intlxpatr |
Adventure, Circle of Life and Death, Family Issues, Health Issues, Survival | Zombies |
Leave a comment

My Mom was concerned; the temperatures are approaching 90°F in Seattle, and most of Seattle does not bother with air conditioning. At night, the temperatures go down into the fifties, cooling everything off, but the day time highs can be more than a little uncomfortable.
“How do you manage?” she asks. “I see the temperatures in (nearby) Mobile are in the 90’s almost every day.”
“It’s not that hard; it’s like living in Alaska – or Kuwait,” I tell her. “When it gets cold in Alaska, you dress warmly, you turn on the heat, you stay inside, and when you need to go out, you get into your car in the heated garage, go in your heated car to a heated store, and you come back home. You don’t spend a lot of time outside.”
I do pretty much the same thing I did in Qatar and Kuwait. I get up and do my devotional readings, and on some days I go to my aqua-aerobics class. on other mornings I volunteer. If I need something, I stop at a store on the way home. Sometimes, I clean house, or do laundry. We often go out for lunch, from the air conditioned car to the air conditioned restaurant and back 🙂 In the afternoons, I quilt or I read, or I quilt and I read.
AdventureMan grew up in the South, he is comfortable with the heat and the humidity. He works out in his gardens; once the temperatures go over 80° I rarely even visit the gardens, maybe when October comes and the temperatures drop. Yesterday morning I looked out as the sun was rising over the gardens and all I could see was swarms of insects rising. I don’t think they were mosquitoes, they looked like little no-see-up kind of things, all speeding around in the rising sun. I don’t do insects, the same way I really don’t do heat and humidity.
The Qatari Cat loves the heat. Part of his daily routine is to eat, then to go into the garage and sleep on one of the cars. It’s like an oven in the garage; it must remind him of living on the streets of Qatar when he was just a tiny thing. He is no longer a tiny thing. When we have international guests over for dinner, they always ask to take photos of him; he has grown to be a very long, tall cat, kingly but gracious.
Yesterday morning, as I headed out, there was a hint of – well, it was not coolness, but it was just not blasting me with heat. It was a respite from the relentless heat. I don’t begin to think it was a hint of winter to come; the summer torment has really just begun and is unlikely to end before late October, but I treasure even a hint of “not a blast of heat.”
AdventureMan asks me if I miss Seattle. Not so much, really, traffic has gotten so bad there, but I miss the climate. I feel energized by the cool mornings, even rain doesn’t bother me. I love the sound of the wind whistling around, I love taking a walk along the waterfront after lunch or dinner. I don’t find it at all surprising that diabetes is associated highly with countries with hot climates; heat makes you lethargic, inactive, all the things that encourage sloth.
Torrential rains are forecasted for this 4th of July weekend; in Pensacola there is a possibility they will diminish just in time for the fireworks. Hmmm. Heat. Humidity. Mosquitoes . . . I love fireworks . . . weighing my options 🙂
July 3, 2013
Posted by intlxpatr |
Alaska, Cross Cultural, Cultural, Exercise, ExPat Life, Health Issues, Kuwait, Living Conditions, Pensacola, Qatar, Qatteri Cat, Random Musings, Weather |
Leave a comment

I didn’t expect to like this book as much as I did; from the first chapter I was hooked, so hooked I didn’t want to go to water aerobics of go to sleep until I had finished it. The title sounds girly and romantic, big yawn, but the book is anything but. The book is tough, and edgy, and tackles the foster care system without using sexual assault or out-of-the-ordinarily-cruel foster parents to bludgeon the point. She botches her one great chance at happiness when she sabotages her adoption by Elizabeth, who loves her dearly. The system can even be caring, but the effect of warehousing unwanted and neglected children damages their ability to trust, and to form relationships. We watch her as a child, self-destructive, angry, undermining her own chances of happiness.
Victoria even has a girly name to go with the title, but she is tough, and self-reliant, and very, very vulnerable, in spite of her toughness. Aging out of the system, she emerges a waif, with a hunger that stems more from emotional needs than physical.
She is greatly blessed to cross paths with people who look at her and truly see her, see her possibilities and her vulnerabilities, people who are willing to work with her, even to love her patiently, in spite of her prickliness and tendency to push people away. One of these is a florist, Renate, who recognizes in Victoria a gift for floral arrangement and is willing to work around her eccentricities. She gives Victoria a part-time job, in which Victoria flourishes.
In her emotional life, however, Victoria still has a lot of unresolved issues, stemming back to the very beginning when she was given up by a mother who, for whatever reason, didn’t want her. While she is hungry for love, she fears it as much as she wants it. Relationships overwhelm her. She abandons the love of her life, and then has to live with the consequences.
Watching her resolve her issues is cliff-hanging. You can’t stop reading. It’s not like watching a train-wreck; you know this girl has inner resources she has not yet tapped; you can read it in the loving evaluation of those who surround her. Every page of the way you are rooting for her to succeed.
July 1, 2013
Posted by intlxpatr |
Books, Character, Circle of Life and Death, Cultural, Family Issues, Fiction, Health Issues, Living Conditions, Mating Behavior, Parenting, Social Issues |
Leave a comment
This is a shock; thank you Hayfa for this up-to-the-minute article from the New York Times. Contrary to all we’ve believed for many years, taking some vitamins – including C and E – shortens your lives. Who knew??
PHILADELPHIA — LAST month, Katy Perry shared her secret to good health with her 37 million followers on Twitter. “I’m all about that supplement & vitamin LYFE!” the pop star wrote, posting a snapshot of herself holding up three large bags of pills. There is one disturbing fact about vitamins, however, that Katy didn’t mention.
Derived from “vita,” meaning life in Latin, vitamins are necessary to convert food into energy. When people don’t get enough vitamins, they suffer diseases like scurvy and rickets. The question isn’t whether people need vitamins. They do. The questions are how much do they need, and do they get enough in foods?
Nutrition experts argue that people need only the recommended daily allowance — the amount of vitamins found in a routine diet. Vitamin manufacturers argue that a regular diet doesn’t contain enough vitamins, and that more is better. Most people assume that, at the very least, excess vitamins can’t do any harm. It turns out, however, that scientists have known for years that large quantities of supplemental vitamins can be quite harmful indeed.
In a study published in The New England Journal of Medicine in 1994, 29,000 Finnish men, all smokers, had been given daily vitamin E, beta carotene, both or a placebo. The study found that those who had taken beta carotene for five to eight years were more likely to die from lung cancer or heart disease.
Two years later the same journal published another study on vitamin supplements. In it, 18,000 people who were at an increased risk of lung cancer because of asbestos exposure or smoking received a combination of vitamin A and beta carotene, or a placebo. Investigators stopped the study when they found that the risk of death from lung cancer for those who took the vitamins was 46 percent higher.
Then, in 2004, a review of 14 randomized trials for the Cochrane Database found that the supplemental vitamins A, C, E and beta carotene, and a mineral, selenium, taken to prevent intestinal cancers, actually increased mortality.
Another review, published in 2005 in the Annals of Internal Medicine, found that in 19 trials of nearly 136,000 people, supplemental vitamin E increased mortality. Also that year, a study of people with vascular disease or diabetes found that vitamin E increased the risk of heart failure. And in 2011, a study published in the Journal of the American Medical Association tied vitamin E supplements to an increased risk of prostate cancer.
Finally, last year, a Cochrane review found that “beta carotene and vitamin E seem to increase mortality, and so may higher doses of vitamin A.”
What explains this connection between supplemental vitamins and increased rates of cancer and mortality? The key word is antioxidants.
Antioxidation vs. oxidation has been billed as a contest between good and evil. It takes place in cellular organelles called mitochondria, where the body converts food to energy — a process that requires oxygen (oxidation). One consequence of oxidation is the generation of atomic scavengers called free radicals (evil). Free radicals can damage DNA, cell membranes and the lining of arteries; not surprisingly, they’ve been linked to aging, cancer and heart disease.
To neutralize free radicals, the body makes antioxidants (good). Antioxidants can also be found in fruits and vegetables, specifically in selenium, beta carotene and vitamins A, C and E. Some studies have shown that people who eat more fruits and vegetables have a lower incidence of cancer and heart disease and live longer. The logic is obvious. If fruits and vegetables contain antioxidants, and people who eat fruits and vegetables are healthier, then people who take supplemental antioxidants should also be healthier. It hasn’t worked out that way.
The likely explanation is that free radicals aren’t as evil as advertised. (In fact, people need them to kill bacteria and eliminate new cancer cells.) And when people take large doses of antioxidants in the form of supplemental vitamins, the balance between free radical production and destruction might tip too much in one direction, causing an unnatural state where the immune system is less able to kill harmful invaders. Researchers call this the antioxidant paradox.
Because studies of large doses of supplemental antioxidants haven’t clearly supported their use, respected organizations responsible for the public’s health do not recommend them for otherwise healthy people.
So why don’t we know about this? Why haven’t Food and Drug Administration officials made sure we are aware of the dangers? The answer is, they can’t.
In December 1972, concerned that people were consuming larger and larger quantities of vitamins, the F.D.A. announced a plan to regulate vitamin supplements containing more than 150 percent of the recommended daily allowance. Vitamin makers would now have to prove that these “megavitamins” were safe before selling them. Not surprisingly, the vitamin industry saw this as a threat, and set out to destroy the bill. In the end, it did far more than that.
Industry executives recruited William Proxmire, a Democratic senator from Wisconsin, to introduce a bill preventing the F.D.A. from regulating megavitamins. On Aug. 14, 1974, the hearing began.
Speaking in support of F.D.A. regulation was Marsha Cohen, a lawyer with the Consumers Union. Setting eight cantaloupes in front of her, she said, “You would need to eat eight cantaloupes — a good source of vitamin C — to take in barely 1,000 milligrams of vitamin C. But just these two little pills, easy to swallow, contain the same amount.” She warned that if the legislation passed, “one tablet would contain as much vitamin C as all of these cantaloupes, or even twice, thrice or 20 times that amount. And there would be no protective satiety level.” Ms. Cohen was pointing out the industry’s Achilles’ heel: ingesting large quantities of vitamins is unnatural, the opposite of what manufacturers were promoting.
A little more than a month later, Mr. Proxmire’s bill passed by a vote of 81 to 10. In 1976, it became law. Decades later, Peter Barton Hutt, chief counsel to the F.D.A., wrote that “it was the most humiliating defeat” in the agency’s history.
As a result, consumers don’t know that taking megavitamins could increase their risk of cancer and heart disease and shorten their lives; they don’t know that they have been suffering too much of a good thing for too long.
<nyt_author_id>
Paul A. Offit is the chief of the infectious diseases division of the Children’s Hospital of Philadelphia and the author of the forthcoming book “Do You Believe in Magic?: The Sense and Nonsense of Alternative Medicine.”
June 25, 2013
Posted by intlxpatr |
Health Issues, News |
Leave a comment
Honestly, who would want to be King? All those events and ceremonies, living your life in a fishbowl? Never a week went by in Doha without rumors of a new wife, speculation about an old wife, and comments on the Emir’s appearance. He has ushered Qatar through perilous times; few “blessings” are as two-sided as new wealth. He is looking healthier and happier than I have ever seen him; maybe he is looking forward to a life of privacy and leisure 🙂 We wish him well; we wish him safety and health and all good things. From today’s Doha News:
Sheikh Hamad bin Khalifa al Thani, the Emir of Qatar, will meet with members of the ruling family and several Qatari advisors today, government-funded channel Al Jazeera reports.
Over the past two weeks, several foreign diplomats have said that a transition of power in Qatar is imminent.
Citing “trusted sources” regarding its information about Monday’s meeting but not elaborating any further, Al Jazeera implied that the talks would revolve around the Emir’s succession plans.
Details about the upcoming changes in government are unclear. But the Emir is expected to cede power to his fourth son, 33-year-old Heir Apparent Sheikh Tamim bin Hamad Al Thani, while the Prime Minister/Foreign Minister, Sheikh Hamad bin Jassim Al Thani, is said to be stepping down.
If the reports are true, the succession would be a historic event for Qatar and the Middle East, a region where rulers normally reign until death.
According to AFP:
“The emir is convinced that he should encourage the new generation. He plans to transfer power to the crown prince, Sheikh Tamim, and to carry out a ministerial reshuffle to bring a large number of young people into the cabinet,” a Qatari official told AFP on condition of anonymity.
The Emir himself was a young 43 years old when he took power from his father in a bloodless coup on June 27, 1995, according to the Amiri Diwan’s website.
Though Al Jazeera’s report came in around 1am Monday, online reaction has already been building, with many Qataris expressing sadness about the potential end of Sheikh Hamad’s rule.
UPDATE | 12:20pm
Two hashtags in English and Arabic, #ThankYouHamad and #شكراً_حمد, expressing gratitude for the Emir and his rule are trending in Qatar on Twitter.
Read more: http://dohanews.co/post/53723624652/report-qatars-emir-to-meet-with-ruling-family-members#ixzz2X8XZKABA
June 24, 2013
Posted by intlxpatr |
Bureaucracy, Character, Civility, Community, Doha, ExPat Life, Family Issues, Health Issues, Interconnected, Leadership, Living Conditions, News, Political Issues, Qatar, Work Related Issues |
Leave a comment